Understanding Ulcerative Colitis
Ulcerative colitis (UC) is a type of inflammatory bowel disease (IBD) that causes inflammation and ulcers (sores) in the lining of the large intestine (colon) and rectum. Unlike Crohn's disease, UC only affects the colon and occurs in a continuous pattern.
Please consult a gastroenterologist for proper diagnosis and management of inflammatory bowel disease.
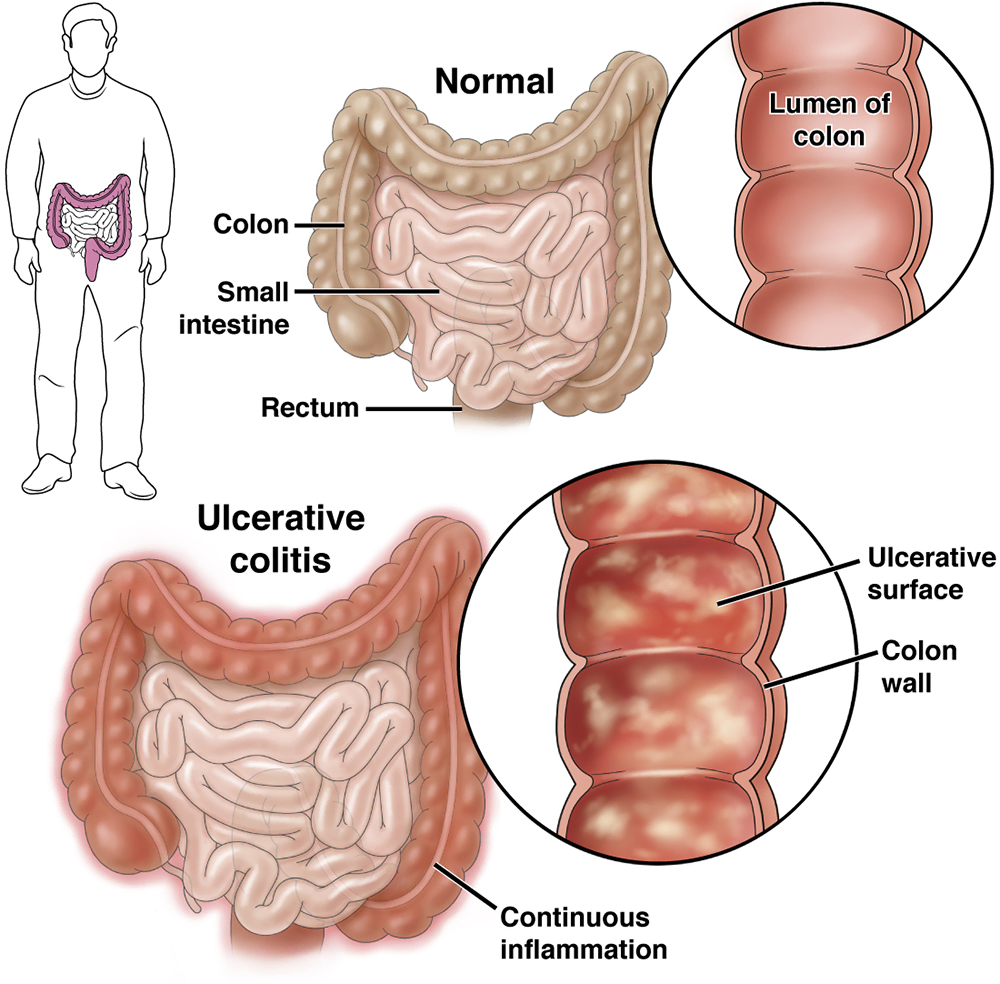
Image Source: Image courtesy of American Gastroenterological Association (AGA). View Source
Comprehensive Treatment Options
Mild to Moderate UC
Aminosalicylates (5-ASAs) - First-line therapy
- Mesalamine (Asacol, Pentasa, Lialda, Apriso)
- Sulfasalazine (especially if joint symptoms)
- Available as oral tablets, enemas, or suppositories
- Anti-inflammatory effects specific to the colon
Moderate to Severe UC
Corticosteroids - For acute flares
- Prednisone (oral) for systemic disease
- Budesonide MMX (Uceris) - targeted colon release
- Hydrocortisone enemas for left-sided disease
- NOT for long-term maintenance
Biologics - For moderate-severe or steroid-dependent disease
- Anti-TNF agents: Infliximab (Remicade), Adalimumab (Humira), Golimumab (Simponi)
- Anti-integrin: Vedolizumab (Entyvio) - gut-selective
- Anti-IL12/23: Ustekinumab (Stelara)
- Anti-IL23: Mirikizumab (Omvoh)
Advanced Therapies
JAK Inhibitors - Oral targeted therapy
- Tofacitinib (Xeljanz) - FDA approved for UC
- Upadacitinib (Rinvoq) - recently approved
- Filgotinib - approved in Europe
Immunomodulators - Steroid-sparing agents
- Azathioprine (Imuran), 6-Mercaptopurine (6-MP)
- Methotrexate (less commonly used in UC)
- Often combined with biologics
Severe/Hospitalized UC
- IV Corticosteroids - Methylprednisolone or hydrocortisone
- Rescue Therapy - If steroids fail
- IV Cyclosporine
- IV Infliximab
- Urgent colectomy if medical therapy fails
Maintenance Therapy
- 5-ASAs - Most patients can maintain on mesalamine
- Biologics - For those who needed them for induction
- Immunomodulators - Often used in combination
Treatment plans are individualized based on disease severity, extent, and patient factors. Close monitoring with your IBD specialist is essential.
Treatment Information: For comprehensive IBD treatment information and resources, visit the NIDDK Ulcerative Colitis Treatment page.
Resource: Public domain medical information from National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), NIH.
Surgical Options
When Surgery is Considered:
- Medically refractory disease (failed all medications)
- Dysplasia or colorectal cancer
- Severe acute colitis not responding to medical therapy
- Perforation, massive bleeding, or toxic megacolon
Surgical Procedures:
Total Proctocolectomy with IPAA (Ileal Pouch-Anal Anastomosis)
- Removes entire colon and rectum
- Creates internal pouch from small intestine
- Maintains continence and avoids permanent ostomy
- "Gold standard" for young, healthy patients
Total Proctocolectomy with End Ileostomy
- Permanent ileostomy bag
- Best option for older patients or those with anal dysfunction
- Simplest procedure with lowest complication rate
Total Colectomy with Ileorectal Anastomosis
- Rarely performed due to cancer risk in remaining rectum
- Only if rectum minimally involved
Important Considerations:
- Surgery can be curative for UC (unlike Crohn's)
- IPAA has 90-95% long-term satisfaction rates
- Fertility may be affected in women (discuss timing)
- Pouchitis occurs in 30-50% of patients with IPAA
Surgical decisions require thorough discussion with experienced IBD surgeons and gastroenterologists.
When to Call Your Doctor
- Persistent symptoms despite medication
- Blood in stool or signs of severe anemia
- High fever, dehydration, or weight loss
- Signs of complications like perforation, toxic megacolon, or colorectal cancer
Final Takeaways
- UC is a lifelong condition, but with proper treatment, many people live full and active lives
- Early diagnosis and treatment can prevent complications
- Regular monitoring (including colonoscopies) is important to assess disease control and screen for cancer
This information is for educational purposes only. Maintain regular follow-up care with your IBD specialist for optimal long-term health management and cancer surveillance.
Patient Resources & Support
Connect with organizations, support groups, and resources for Ulcerative Colitis:
- Crohn's & Colitis Foundation - Support, education, and research
- IBD Patient Support - Build your IBD care team
- My Crohn's and Colitis Team - Social network for IBD patients
- IBD Meal Planning - Gut Friendly Recipes
Medical Disclaimer
This content is for educational purposes only and is not intended as medical advice. Always consult with a qualified healthcare provider for diagnosis and treatment of medical conditions.
References
- Ungaro R, Mehandru S, Allen PB. Ulcerative colitis. Lancet. 2017.
- Rubin DT, Ananthakrishnan AN, Siegel CA. ACG Clinical Guideline: Ulcerative Colitis in Adults. Am J Gastroenterol. 2019.
- Harbord M, Eliakim R, Bettenworth D. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. J Crohns Colitis. 2017.
- Feagan BG, Rutgeerts P, Sands BE. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013.
- Sandborn WJ, Su C, Sands BE. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2017.
- Lightner AL, Mathis KL, Tse CS. Postoperative outcomes in ulcerative colitis following restorative proctocolectomy with ileal pouch-anal anastomosis. Ann Surg. 2017.
- Fazio VW, Kiran RP, Remzi FH. Ileal pouch anal anastomosis: analysis of outcome and quality of life. Ann Surg. 2013.
- Turner D, Walsh CM, Steinhart AH. Response to corticosteroids in severe ulcerative colitis. Clin Gastroenterol Hepatol. 2007.
- Farraye FA, Melmed GY, Lichtenstein GR. ACG Clinical Guideline: Preventive Care in Inflammatory Bowel Disease. Am J Gastroenterol. 2017.
- Lutgens MW, van Oijen MG, van der Heijden GJ. Declining risk of colorectal cancer in inflammatory bowel disease. Inflamm Bowel Dis. 2013.